Introduction
Intra-op microrecording/microelectrode-recording (MER)1 has been established to advance objective site throughout stereo tactic-surgical-operation.2, 3, 4 Benabid developed a holder with five parallel channels for micro/macro needles. 5, 6, 7 The needle for MER, which is incorporated in the electrode for test stimulation, is able to pick up electrical activity ofneurons within the proximity of the electrode because of its tiny angle. MER signals of STN spike-patterns designed for STN neurons located whichever within STN or in the globlal pallidal (GP) are quality-attributes, plus looks different as of neural/neuronal signal-spike-patterns of the neighboring anatomical-structures which makes the chance to discriminate the boundaries and limits of both aimed-structures.8, 9, 10, 11, 3, 12, 13, 14, 15, 16, 17 In addition, within sub thalamic nucleus pallidal neurons, adiversity-of-neurons, also sub structures might be documented familiar and predictable which separate functionally dissimilar regions. 18, 19, 20, 21, 22, 23, 24, 25, 26, 27
Even though microrecording discloses electrical-activity as well as signature-patterns of dissimilar sub structures-of-brain, it`s hard and complicated and complex to decide whether microrecording has the `positive-outcome` over the clinical finding of stimulations with deep brain stimulators therapeutic procedure.28, 29 Eventually, in the due course it might be significant to find-know whether application of the microrecording has a +Ve result over clinical findings plus whether pressure that the microrecording has had over the alternative option of objective which has been valuable and helful. Though these queries are quite problematica to respond it is because the diagnosis and clinical-prognostic finding is unwavering and single minded through several indeed many more factors than the use-of-microrecording alone`. Hence, which does not been aim-of present-study. Therefore, as the initial outcome of this `longitudinal-study` over the microrecording of the STN neural signals while the dee brain stimulators are `ON`. This was experimented to what extent application of microrecoring influences and impact the dee brain stimulators operational process (DBS neuro surgical-procedure). The comparative and virtual input of the physio logical-data achieved through the microrecording as well as diagnosis prognosis-clinical (diagnostic and prognostic) data obtained by intra op test stimulus to the assortment-of end-point for embedding the microelectrodes implantation was assessed. In addition, we observed to what extent, the behavioral-activity signature/pattern achieved through the microrecording characterized by the site or effectiveness of lead-point-based exclusively over the (3D-MRI). In conclusion, lastly, it was examined whether the objective lead-point depending on the finest recording, i.e., microrecording behavioral-activity coordinated and harmonized the lastly selected point for the macro-lead and microelectrode implantation depending on the intra op test stimuluses.
Materials and methods
Parkinson disease Patients-demographic’s
Since last four years, fifty-even successive and uninterrupted advanced idiopathic Parkinson diseased subjects (diseased patients) those who underwent the D B S within the sub thalamic nuclei, i.e., the S T N – D B S, plus twenty-eight uninterrupted PD-conditions (subjects who are patients diseased conditions) through whichever dystonic-movement disorder (size of the population `n=23`) and/or Pakinsonians (Parkinson’s disease, whose population size `n=5`) in whom the inner section of G P i- D B S was aimed were clubbed.
The data of the t w o of the sub thalamic nuclei conditions /patients couldn`t be employed because, within the patient through the bi lateral (/ two-sided left and tight hemispheres of the brain) implant, merely movement-activity as of the `central-channel-electrode` was acquired/recorded, plus in one more patient, a huge exterior electrical-stimulus artifacts/noise distortions were occurred. Within the twelve Parkinsonians, the operation was accomplished uni-laterally (one side). Which builds and creates (two sides and 46 patients) sub thalamic nucleuses-sides. The data of the three3 G P I neural patients couldn`t be employed because, in 1 single Parkinsonian, simply movement-activity as of middle/central-channel` was acquired/recorded, another Parkinsonian was operated overon through local-anesthesia, also within the acquisitioned-recordings of 3rd Parkinsonian, a huge outside electrical-stimulus noise artifacts were presenting.
In 4Parkinsonians, the neurooeration/surgery was done unilaterally (one-sided) which builds sum of overall forty six incorporations (i.e., implantation of electrode in forty-six Parkinsonian subjects) within Pallidal nucleus. Subjects were informed and obtained the consent intended and designed for the oeration/neurosurgical dee brain stimulation processing which includes support vector machine based microrecording. A few Parkinsonian subjects through the Parkinson’s disease merged within the study and were redicted/randomized to the sub thalamic nucleus and also globaus Pallidus nucleus, i.e., G P I – D B Sas part-of the higher multi center diagnostic-clinical/ and Prognostic test examination (on trial basis).
Addition/insertion or inclusion criterion for the operational-surgery (advanced idiopathic Parkinson’s disease through the invalidation motoric oscillations) plus elimination criterion (psychosis, cognitive dementia CD, cognitive impairment CI, hallucinations, memory issues, severe depression,/dementia, and universal normal wide-ranging contra indications for the neurosurgery) were the identical and equal for diseased patients, i.e., Parkinsonians allotted to the sub thalamic nucleus dee brain stimulations and global pallidal neurons dee brain stimulators implantations, as well as for the Parkinsonian subjects who are patients and who is not participate in test examinations. Local anesthesia to all the subjects were given by the authorized anesthetist only.
Deep brain stimulation technique
In this experiment the D B S technique is as follows. It’s a bi lateral means subject wo sided procedure and by applying the C R W frame-based three-dimensional imaging (3D-MRI) restorations aimed for computing plus directional-path-development, and by applying the microrecording and macrostimulation techniques.
The aimed-target co-ordinates applied were “12m ms” horizontal to standard plane of t h i r d ventricle, “2mm” subsequent/later-posterior to the mid commissural point (i.e., the MCP-point), and 4m m below the inter-commissural line (i.e., theICL) intended for s-nucleus, 21mm adjacent to the standard plane, 2mm forward (frontal) towards the M C P, 5mm beneath I C L aimed at pallidal neurons. Modifications were done depending on the graphical-image structure over the intending imaging (i.e., the M RI) in case needed. The directional-paths/directions aimed at central-electrode-channel were well-defined and demarcated through subsequent criterion: forward, i.e., frontal(anterior or forehead)angulation towards the I C L of the degrees from fifteen to twenty (15°–20°), adjacent/lateral-angulation as of mid – line(20°–30°) entrance (pass-entry) over the gyrus, plus sidestepping ad a thin line in the filed called ‘sulci’, c o r ti c a l- s u r f a c e veins, as well as side-ventricles`. Inside the bi lateral-cases, neurosurgical operation began over the left side of the Parkinsonian. 3to5 brace (steel) cannulas as well as micro electrodes were incorporated via a 12mm distance pre-coronal “burr-hole” which is very thin.
Each and every cannula`s keep on put off in dwelling during the neuro-operational-surgical procedural-process to scotch or stop the brain shift throughout, all through the DBS neurosurgery as well as prevention selecting the incorrect zone throughout embedding the end-channel-electrode. The electrodes were made by the Ms.Medtronic and their models are3389 by 4platinum/iridium cylinder-shaped exteriors (whose diameters are:1.3m m plus lengths are: 1.5m m) also through the inner link split of 0.5m ms. The Link’0’ is distal, plus link’3’ is highly-proximals. Since it was local anesthesia given and hence each and every patient was awakened also none were with the impact of narcotics, or tranquillizers, or downers (i.e.,sedatives). DBS neuro-surgery as well as microrecording was done understanding nightlong removal of the medicine (anti-Parkinsonian). For the verification of the effectiveness of the lead/electrode point, subjects undertook post op CRW-frame-based stereo tactic post op MRI imaging.
Microrecording procedure
For performing the microrecording at the extra cellular levels sole /single neuron multi unit microrecording is done through miniature (10μicron meters thickness) micro recording signals of the s-nuclei and global pallidal neurons were acquired though biomedical instrumentation/ differential amplifiers, nearly ten thousand-times amplified. Medtronic lead point machine with the boot strapping mechanism as well as referent band pass categorized amongst 0.5kHz-5kHz(−3dB;12dB/oct). All the waveforms were done with 12kHz-sampling frequency, i.e., sampled@12kHz. An analog to digital conversion card is employed whose dynamic range or pixel resolutions were16-bit then it was up sampled to the frequencies of24kHz. 2 seconds signal steadiness interval following the microelectrode passage interruption, multi neural sections acquired for the duration of five to twenty seconds (5s-20s).
Launching for the s-nucleus as well pallidal neurons eight and twelve millimeters (8mm-12mm) over the MR imaging-based goal, and then micro electrodes advanced within the steps-of five-hundred(500μm) to the goal via the human intervention micro drive. Once electrodes on the s-nuclei and pallidal (GPi,e) neurons zones at every distance or intensity, the s p i k i n g movement and behavioral-activity of those neurons sitting and situated within the proximity to the needle-electrodes, the pick up regional-zone upto200μm) can be acquired/recorded. Rest on the neural-density not >3units – >5units acquired asynchronously. However, those isolated and far away-units couldn`t be differentiated as of back ground signal-levels.
In connection with the intensity of embedding microelectrode within the s-nuclei stimulations through the deep brain stimulators, it`s a practice to embed the interaction connection numeral one (1) at point-location through the finest “stimulus-parameters”, via through the cordial connection two2mm beneath this ‘ideal-point’.
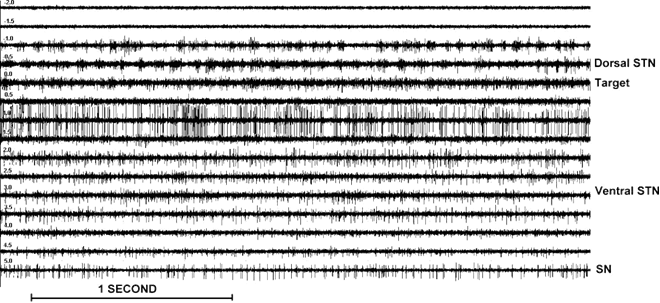
Figure 1
Sub thalamic neural movement and behavioral-activity for differentintensities:−2 and +5m m). Observe the minus readings relate to locational-points over the aimed region of STN. Insignificant s t n region−1 and 0m m) is distinctly established through the upsurge and inside and afterwards related-noise` as well as an abrupt rise within the rate-of-discharge (emitting)characterized by rhythmic bursts of activity in this case from 15 to 25 Hz. Deeper layers of the STN (+1.5 to 3.5 mm) show a more irregular high-frequency discharge pattern. SN activity (+5 mm) consists of a low-frequency tonic discharge.
Results
As per the electrode implantations and in all five channel electrodes, at any rate maximum in a channel there is microrecording activity and movement behavioral wise (as showed in Figure 1, Figure 2). Within the subthalamic-nucleus brain neurons, out of ninghty eight(98) cases, i.e., 9%, only nine (9) cases, i.e., (9/98), there was no recording activity within the cantrelchannel. Similarly, out of forty eight (48) cases, in (1), i.e., 2%, there was no microrecording activity and movement and thus behavioral aspect in the centralchannel and so its difficult to judge or conclude.
The tables1 pertaining to the (STN) computational data as well as table2 pertaining to the (GPi) depict the `frequency-allocation` of the final-choice forever the channel-electrode interfacing with the central, lateral, medial, (frontal)anterior, or exterior(posterior) channels derived from and founded on microrecording also macro stimulation test with DBS stimulations, and the allocation of the electrode -channels within which, the finest best recording was observed, i.e., the longest trajectory through the S T N and/or G P i neural/(neuronal) behavioral-activity. The middle one only was chosen, i.e.,central channel for embedding the electrodes forever within the sub thalamic nucleus-STN(50%) as well as in globus pallidal neuralGPi(57%). And also in sub thalamic nuclei-STN 64%cases, the channel electrode through the finest microrecording activity and behavior was selected for interfacing the electrodes forever. Similarly, in global alliduss neurons nuclei 61% cases, the channel electrode through the finest micro recording activity and behavior was selected for interfacing the electrodes forever.
The effectiveness of end electrode within the sub thalamic nucleus, was added frequently tangential, i.e., on the side/imaginative than medial to computationally aimed, 10%, i.e.,(10/98 tangential, and6%, i.e.,(6 / 98) medial also repeatedly frontal(anterior)24%, i.e.,(22/98) than the exterior, i.e., posterior(10% , i.e., (10 / 98), and or otherwise implanted within the middle, i.e., central.
The finest microrecording in sub thalamic nucleus was examined tangential (peripheral at a tangent and divergent) than medial plus higher frontal(anterior) than the exterior(posterior) as of the computed objective (i.e., determined target). The end-electrode point for globus pallidus has had propensity and predisposition to move laterally higher than medially. Even though in pallidal nucleus, the microrecording was maximum at the lateral(posterior) channel-electrode in 9 out of 46 cases, i.e., 20%cases, and because of dyskinesias, through the macrostimulation testing stimulations in 2of 9cases only, this channel-electrode was chosen for the stimulations forever. The frontal-channel electrode was applied very hardly ever, and also seldom. In bilaterally operated STN-DBS patients, The middle one was selected for embedding the end-electrode in the left brain(50%STN) sub thalamic nucleus as well as right side brain (39%STN) yet statistically insignificant p<=0.42 within the two sided electrode implantations performed in sub thalamic nucleus region with the stimulations through the deep brain stimulators. Likewise, the two sided bilateral brain, in the Parkinsonians was performed within the globus pallidal nucleus and the middle-central was selected for interfacing the end-electrode (82%in the left pallidal nucleus, 65%in the right-hemisphere pallidal nucleus. However, the p value was insignificant statistically, p<=0.37.
Table 1
Comparison between the channel with the best MER Activity and the channel finally chosen for permanent stimulation in the STN.
Table 2
Comparison between the channel with the best MER activity and the channel finally chosen for permanent stimulation in theGPi
The last and final(end) intensity of embedding or interfacing virtual to the imaging-based objective is shown in this experimental investigation (Figure 2). In support of the sub thalamic nucleus, the standard intensity of the genuine and earnest touching-point contacting—point for stimulus-electrode2.1mille meters, the standard deviation1.5mille meters, means, implying approximately correct communication flanked by the target-STN computed over the projecting image through the M R I, plus the usual standard (average-mean)point-of-contact was one(1mm), and because of the 2mille meters disparity flanked by the midpoints of two consecutive and succeeding connecting-sites.
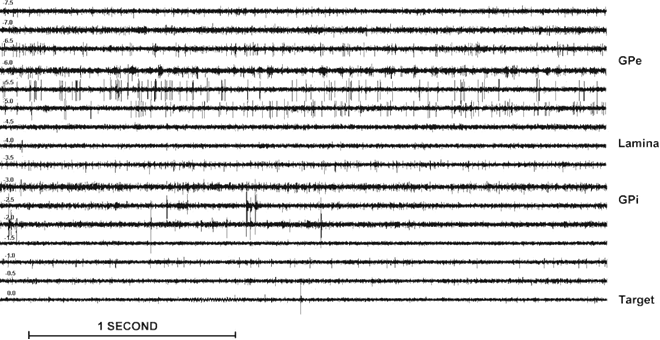
Figure 2
Single/multi-unit activity of global pallidus nucleus intensity`s(−7.5mm and to the 0mille meters).
For globus palliidus nucleus neurons, the earnest and cordial connecting or contacting position embedded over the mean-average approximately at the computed intensity levels (the mean-average=−0.5mille meters and the standard deviation=1.2 mille meters, as shown in Figure 3.(B).
Figure 3
A: Sub thalamic nucleus frequency/sharing or allocation of final intensity of earnest contacting/connecting-point (mean=2.1mille meters, the standard deviation was 1.5mille meters) with regard to the magnetic resonance based imaging objective
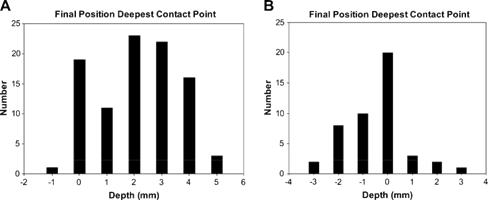
Figure 4
A: The frequency allocation of sub thalamic nucleus center of microrecordinng activity and behavior through in regard to magnetic resonance based objective image of s-nuclei B: `Scatter-plot` of connection among sub thalamic nucleus centre of micro recording-activity(parallel) as well as the last and final-end intensity of the earnest contacting-site (perpendicular) in regard to magnetic resonance based imaging objective o the sub thalamic nucleus aimed/target. The nucleus data of right brain as well as left-brain sub thalamic nucleus neurons were pooled.30, 31
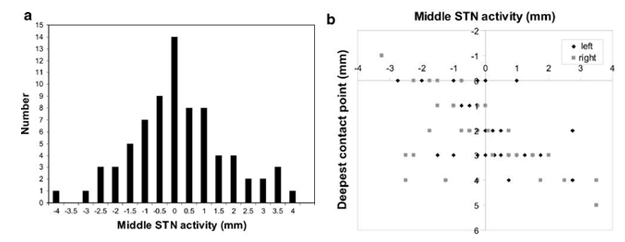
The intensity point of subthalamic nucleus central in regard to magnetic resonance based image objective was computed as of the commencement or start plus end-of s-nuclei and microrecording movement/activity of the M E R belongs to the electrode-channel which has had the finest movement and activity by of the microrecording. The average of frequency-allocation was0.0mille meters by the standard deviation of 1.6mille meters, shown in Figure 4(A). Mutually pooled through the findings illustrated in Figure 3(A), which means, over the mean-average, the contacting-point 1mm was positioned within the center of sub thalamic nucleus.
In Figure 4.(B) showing the contrast among sub thalamic nuclei central plus last and final end intensity interfacing of earnest contacting-site and virtual to magnetic resonance image based aimed objective which is established and confirmed that, a superior-range ±4mille meters for point of sub thalamic nucleus centre point than for lastly selected intensity-levels−1 and upto+5.
Conclusions
This study reveals that, the lastly selected intensity levels meant for the sub thalamic nucleus deep brain stimulations corresponded within the fifty-seven percent (57%) of Parkinsonians through pre operatively magnetic resonance aimed image objective with in the range-of±1mille meters. However, the option of selection of end objective also which of the channel electrode point given best ` t h e r a p e u t i c – w i n d o w` was supervised through microrecording activity-movement plus lastly resolute through the findings of intra op testing stimulations through the deep brain stimulators. 32, 33, 34, 35, 18, 12, 13, 36, 14, 24, 25, 37
According to the microrecording activity within the sub thalamic nucleus multi site multi-electrode multiple-channels, the early choice shall be done such that which channel-electrode might be absolute candidate for the final testing’s of macrostimulations -testing`s through the deep brain stimulations plus at what levels and at what intensities must be enthused. 38, 39, 40, 28, 30, 31