Introduction
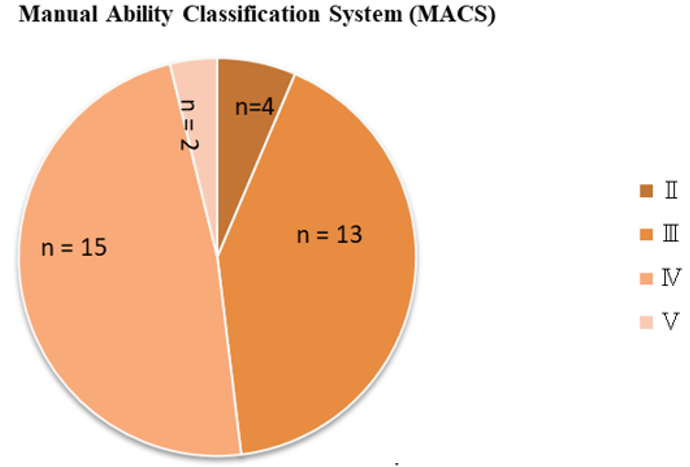
Cerebral Palsy (CP) is defined as the impairment of movement and posture development, it is a group of disorders that affects children’s ability to move and maintain balance–posture, restricts activities because it is permanent, non-progressive disorders in the developing fetus or infant brain.1 CP is common motor disorder in early childhood which is due to multifactorial aetiology like congenital, genetic, traumatic, infectious and metabolic with any of prenatal or postnatal period and it is associated with motor function difficulties, including muscular weakness and poor balance, coordination and posture.2 Neurological problems are accompanied by muscles weakness, Abnormal Muscles tone, Balance Problem, Loss of Selective Control, Loss of sensation, Pathological Reflexes, Swallowing problems, perception, cognitive, communication and behavioural problems, with Epilepsy, Visual Problem, Hearing Loss, Feeding Difficulty with failure to thrive, Respiratory Problems and secondary musculoskeletal system problems like Contracture and Deformities are seen in CP. Postural control is the way of Central Nervous System which regulates sensory information from other system in order to produce adequate motor output to maintain a upright posture, it is ability to hold the centre of gravity within the base of support, without worsening in the balance. The trunk control is the ability of trunk muscles to allow the body to remain upright, adjust weight shift, and performs particular movements of the trunk so as to maintain the centre of body mass within base of support during static and dynamic postural control, so far trunk has an important role in the maintaining of postural control and balance reactions.3 In CP Postural Control is a one of the problem especially, thoracic kyphosis is excessively increased to compensate for the characteristic posterior pelvic tilt and another cause of compromised posture is due to abnormal muscle tone and muscle imbalance which is evident in subjects with CP.4 Motor difficulties interfere with targeted movement and also activities of daily living such as reaching, grasping, upper body movements due to exaggerated reflexes, Hypo-tone or spasticity of limb and trunk, abnormal posture, involuntary movement or some combination of these.5 Of these, Manual Ability Classification System is a five-level classification which classifies the manual ability of children with CP class on basis of self-initiated ability to manipulate objects in the home, school, and community. Children at level I can perform all manual tasks and can handle objects easily and successfully, whereas children at level V are completely dependent and demonstrate very limited ability in performing even simple actions. It is determined by a parent or caregiver who regularly observes the child’s functions in daily life, in collaboration with a health care professional. The trunk also provides for free movement of the arms and the hands by balancing within the base of support. 3 Children with any type of CP have difficulty in maintaining static or dynamic trunk control, which may directly leads problem with sitting control and standing skills, also it will one of the cause for activities limitation such as reaching, object hand manipulation, Fine motor, upper body co-ordination and walking.6 Difficulties in upper extremity function is most common in children with CP. The Children with CP are more challenged by manual dexterity such as gripping (power/precision) or object handling, which are important in daily activities. Problem in maintaining trunk control and posture there are difficulties in performing in tasks can be caused by an inadequate active motion of upper body, reduced power or precision grip strength and persistent primitive grip reflexes. The trunk has important role in voluntary upper extremity movements and functions, including motor control and motor skills.7 Trunk is important for children with CP due to motor problems to use their hands to support themselves in sitting, standing, and walking, or to transfer themselves anywhere will compromised. Proper upper body functioning along with trunk control is a critical determinant in the ability to perform and participate in daily activities. For this consequences, it is important thing to understand any relation between trunk control and upper limb functions in children with CP. Upper extremity functioning are good enough when an individual is able to finely control their trunk and maintain posture. 8 Conventionally, there is one tools for evaluating upper limb function are ABILHAND-Kids questionnaire. 9 However, the relationship between trunk control ability and upper limb function in children with CP has interesting and making some little attention. Therefore, Aim of the study was to assess the any correlations between the Trunk Control by using Trunk Control Measurement Scale (TCMS) score, and upper limb functions by ABILHAND KIDS QUESTIONNARIES. This study hypothesized that ability of trunk control would be affect upper extremity function in such children with CP.
Materials and Methods
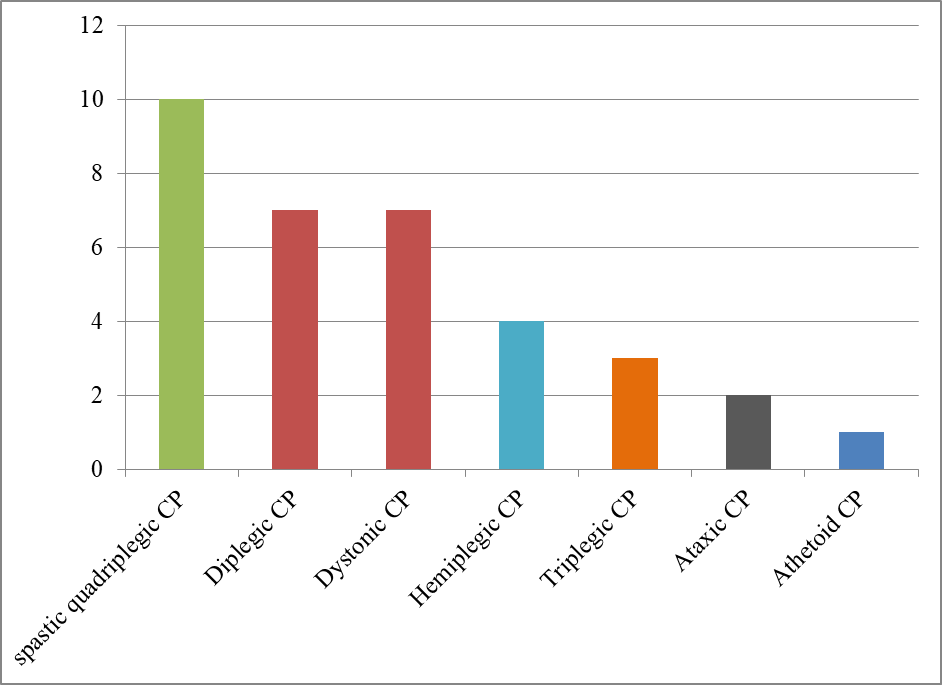
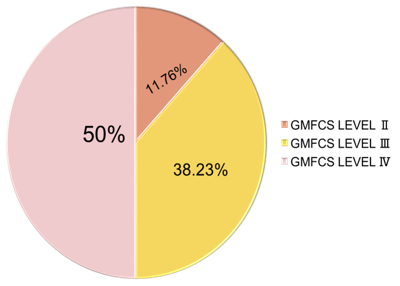
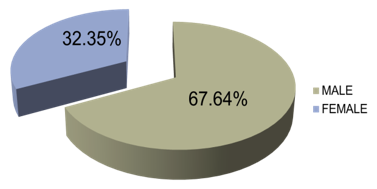
The study was conducted in the neurorehabilitation OPD of SBB College of Physiotherapy, SVP Hospital and private clinics of Ahmedabad. Informed consent form from all parents or caregivers was taken. The estimated sample size was 30. In which 34 children (23 Boys and 11 Girls) aged of 6 to 15 (mean, 8.05 ± 4.5) years were included. The inclusion criteria of this study were: (1) age between 6 to 15 years, (2) Any clinical type of CP (3) CP of level Ⅱ, Ⅲ, Ⅳ as scored after screened by used the Gross Motor Function Classification System; and (4) both boys and girls. The exclusion criteria were: Recent injuries or orthopedic surgery of upper extremity within the last 6 months. As per selection criteria any clinical type of cerebral palsy were subjects were from neurorehabilitation department of SBB college of Physiotherapy, SVP Hospital and Private clinics. After that TCMS for trunk control were checked by primary therapist and ABILHAND Kid Gujarati version questionnaires for Upper Limb Function filled up by parent’s personal interviews.
Outcomes
Trunk Control Measurement Scale (TCMS)
The TCMS was used to assess trunk control during sitting. The scale considers static balance, dynamic/sitting balance, and dynamic reaching. Previous reports found that reliability was excellent; the intra and inter-ratter intraclass correlation coefficients (ICCs) for evaluations of children with CP were 0.87–0.99 and 0.87–1.00, respectively. 10 The TCMS includes 15 items that assess two main components of trunk control: static and dynamic sitting balance. While the total score changes between 0 and 58, higher scores indicate a better level of performance. All children were tested three times and the best score was used in data analysis. A break of about 10 s was allowed between each trial and a 1-min break was allowed between each test.
Abilhand-Kids Gujarati version questionnaire
The Abilhand-Kids Gujarati version questionnaire is used to measure bimanual ability in children with CP. It consists of 21 items exploring daily community activities; all are initially graded as impossible, difficult, or easy. The questionnaire is completed by caregivers. In an evaluation of children with CP, the questionnaire showed a high degree of reliability (r = 0.94) and good reproducibility (r = 0.91). 11
Results
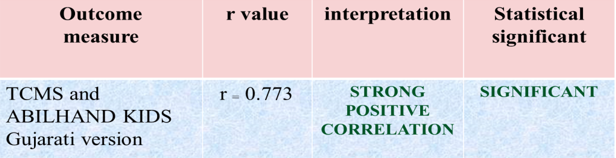
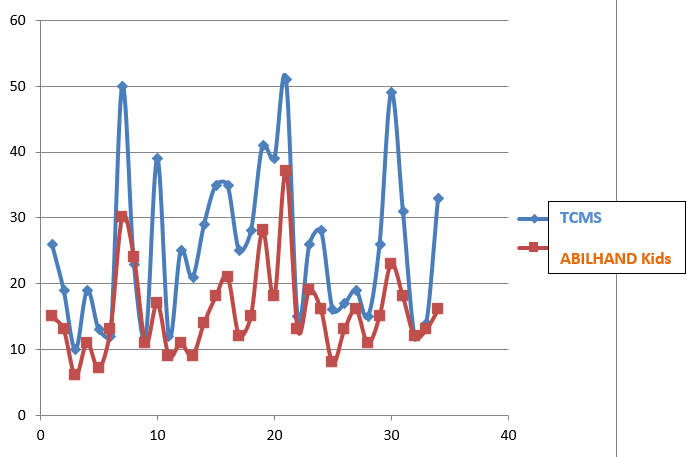
All statistical analyses for 34 subjects were performed using SPSS version 16 and Microsoft excels 2019. By using Kolmogorov smirnov normality test we found that data was not normally distributed. So nonparametric test was used. Correlation coefficients and statistical significances were calculated by the Spearman’s correlation test. p value of ˂0.05 was considered statistically significant. The present study found highly significant correlations between trunk control ability and upper extremity function in subjects with CP. The TCMS scores correlated positively with the ABILHAND-Kids scores (r ₌ 0.773 p ₌ 0.05).
Discussion
The Present study explored that there is relation between trunk control ability and upper extremity function. Trunk control ability assessed by Trunk Control Measurement Scale (TCMS) and used ABILHAND-Kids Gujarati version questionnaires to explore upper body function along with gripping in children with CP. The TCMS scores strongly correlated with the upper limb functions. Trunk control ability in children with CP is different according to their topographic involvement. Literature found that the trunk control was less impaired in hemi paretic CP, more impaired in diaplegic CP and severely impaired in quadriplegic CP.6 Özal et al. reported that children with hem paretic and diaplegic CP had significant differences in TCMS and upper limb functions scores, also that children with unilateral CP had better trunk control along with good upper limb function.12 The some of literature has shown that it is especially important to increase understanding to role of trunk control with their voluntary function and postural control during Neurorehabilitation planning for children with CP. Woodbury et al. had explored the literature on effects of trunk training on upper limb reach and function in patients with chronic stroke sequel. They found that trunk training has better role in improved upper limb functions as arm reach trajectories, shoulder flexion, and the elbow extension range of motion.13 The aim of include another categorized subjects was to know the trunk has vital role in irrespective of Neuro disorder. Also Cherng et al. did study on comparisons of reaching ability between children with CP and healthy children. They explored that the normalized ground reaction force of children with CP (31–53%) was significantly smaller in compare with healthy children (47–61%) during reaching and grasping. 14 Sahinoglu and Coskun also explored that better postural alignment facilitated by adjustable seating significantly improved arm control ability, upper limb function compared with that traditional postural alignment.15 Although Literatures investigating upper extremity functions in CP. They generally focused on unilateral CP and diaplegic CP and concluded that hand function is impaired in CP because of poor trunk control and postural alignment. 16 For this reason, this present study more focused on evaluated trunk control and upper extremity functions in children with any clinical type of CP.
The associated movements caused by inappropriate muscle activation patterns due to significant impact on the development of muscle, it may be progressive tightening, thinning and shortening of muscles often development of muscles contractures and the ability to perform only isolated movements are the main problems with the upper extremities of children with CP because of poor postural alignment.17 This study explored that children with less or poor trunk control have a reduced ability to perform isolated movements of upper extremity along with grip. As a consequence, upper extremity movements are compensated for by involving the trunk. Children with CP often have problem in coordinating their fingers while gripping and releasing their grip.18 Based on the previous study fact that gripping skills may be inadequate in children with CP which have another cause also apart from only trunk control as high or low muscles tone, in this Study assessed gripping skills in children with any clinical type of CP in relation with trunk ability. Study found that there was a relation between trunk control and gripping skills. This study showed that when children with CP have sufficient trunk control they were more successful in performing upper limb activities with releasing and grasping.
Presented study had some limitations also. First, because we focused on children with CP, the sample size was small. Another limitation of this study was that it was a cross-sectional study, and the developments of the children were not followed over time.
Conclusion
The present study concluded that there is a strong positive relation with trunk control ability and upper extremity function in children with any clinical type of CP. Therefore, it is important to focus on trunk control in Neurorehabilitation to improve upper extremity performance along with better postural control.