Introduction
World Health Organization (WHO) defines stroke as “rapidly developing clinical signs of focal or global disturbance of cerebral function, with symptoms lasting 24 hours or longer or leading to death with no apparent cause other than of vascular origin.1 Stroke is the third leading cause of death and one of the most common disabling diseases that has an enormous emotional impact on both patients and their family members.2
Depression is a common psychiatric consequence of stroke with quoted rates of post-stroke depressive disorders ranging from 18% to 61%. Post-stroke depression may affect a patient’s ability to participate in therapy and is associated with slower progress in the rehabilitation and increased length of hospital stay. 3
In the same way, anxiety is also common in post-stroke individuals with the incidence rate being 20%, and it is most common in the first three to four months after the stroke.4 Many studies have shown the relationship between post-stroke anxiety, age and gender. Women and younger individuals are more vulnerable to develop post-stroke anxiety, while another study reports no such relationship. 5
There is a paucity of reports on psychiatric morbidity following a stroke in India, and other developing countries, in general. Hence the present study aims at exploring morbidity of depression and anxiety among stroke patients visiting the General Medicine Outpatient Department in a tertiary care hospital in Mandya.
Materials and Methods
Study Population
This study was conducted in 100 patients who have undergone treatment for stroke and reported to Mandya Institute of Medical Sciences (MIMS), Mandya.
Study method
This was a three months cross-sectional descriptive study in which the data were collected through the method of interviewing semi-structured questionnaire, General Health Questionnaire (GHQ-28) and Hospital Anxiety and Depression Scale (HADS). The study was approved by the Institutional Ethical Committee, MIMS, Mandya. All adult patients who have undergone treatment for stroke in the past 1 month to 3months before the study period reporting to MIMS and who have given informed consent to participate in the study was chosen for the study and patients with aphasia and those with the previous history of psychiatric illness were excluded from the study.
Statistical analysis
The analysis was done descriptively. MS Word and MS Excel was used for entering and analyzing the data. Qualitative variables were expressed as mean, standard deviation, percentage etc. Statistical analysis was done using t-test, chi-square test etc. to detect significant difference or association.
Results
One hundred and thirty eight stroke patients were screened during the study period and 100 were included in the study of those fulfilling the inclusion criteria and who gave informed consent. The clinical and demographic profile of these patients is given in the table-1 and table-2 depicts functional diagnosis of stroke and Figure-1 shows site of pathology. The mean age of the study population was 52.13± 9.4years. Sixty two (62%) patients were showing depressive symptoms as per HADS-D and twenty two (22%) were scored high scores and seven (7%) of them were diagnosed to have Anxiety disorder symptoms as per HADS-A. and none of them were any on psychiatric treatment. When depressed (n=62) and anxiety (n=07) patients were compared to those of other patients who were not, it was noted that depressed patients were mostly low socioeconomic status (<0.001), substance use(<0.001) and had co-morbid illness(<0.001) like DM and HTN.
Depression was not related to parameters like age, education, type of lesion and anxiety was not related to occupation, socioeconomic status and substance use.
Table 1
Clinical and demographic profile of the study population (n=100)
Table 2
Functional diagnosis of stroke
| Side involved | Type | Frequency n=100 | Percentage (%) |
| Rt. | Hemiparesis/Hemiplegia | 33 | 17 |
| Lt. | Hemiparesis/Hemiplegia | 53 | 16 |
| Rt. | Facio-brachial monoparesis | 4 | 4 |
| Lt. | Facio-brachial monoparesis | 10 | 10 |
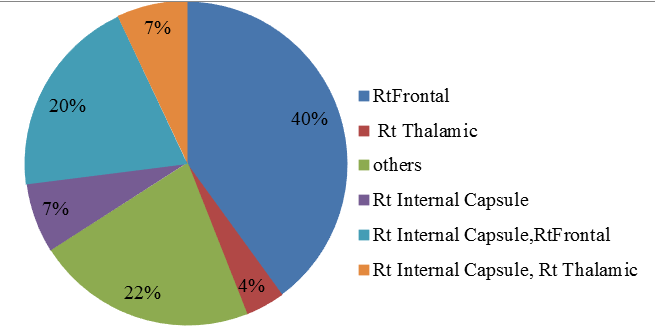
Table 3
Relationship of clinical profile, functional disability with depression
Table 4
Relationship of clinical profile, functional disability with Anxiety
Discussion
The assessment of 100 post-stroke patients’ who reported to the General Medicine Outpatient Department of Mandya Institute of Medical Sciences (MIMS), Mandya were done based on the inclusion criteria to determine the comorbidities of depression and anxiety. Most of them belonged to the older age group with a mean age of 52.3 ± 9.4 years. Majority of them were male patients (57%) while the remaining (43%) were female patients.
We observed that a large number of the people under the study belonged to economically backward class and had low literacy, though it did not reveal any association with the symptomology which is similar to the observations of a study done by Anderson et al (1995).6 which stated that socioeconomic status did not influence the risk for developing post-stroke depression. This could be explained by the geographical distribution of the population and economic status among the people in the state.
When the Neuropsychiatric aspects in post-stroke patients were assessed, the majority of the studies focused on post-stroke depression while the studies about post- stroke anxiety were limited. Our study focused on both the conditions and 54% of the subjects had depression, on the other hand, anxiety was observed in 8% of the study subjects based on the HADS. These observations are similar to the findings of a study conducted by Robinson et al.7
Though abundant researches have been done to study the association between age and post-stroke-depression, our study did not reflect an association between the same. These findings were similar to a study conducted by Robinson and Anderson et al. 6, 8, 9 However, recent studies show that the risk of post-stroke depression is common among younger patients than in the older ones.
Unlike the prevalence of depression among females in the general population, which is high, our study revealed that post-stroke depression was high among the males. Our study results comply with studies conducted by Johnson et al, Ramasubbu et al and Berge et al. 10, 11, 12
We found statistical significance in co-morbid medical illness in post-stroke patients. Majority of the individuals had diabetes and hypertension as a co-morbid condition, this is because these two factors are the major risk for developing stroke I.Alam et al and M.Fayyaz et al. 13, 14
Studies on post-stroke anxiety are limited in numbers compared to that on post-stroke depression. Our study result that the prevalence of the former is 8% is supported by the results of a study conducted by Astrom et al 15 in which the prevalence of the same ranges from 4%-28%.
When laterality is considered, many studies showed various relationships between the side of the lesion and symptomatology. 62% of the subjects had left hemisphere involvement while 38% had a lesion on a right hemisphere which was confirmed by the imaging technique. The current study found no significant association between the frequency of depression and left hemispheric stroke. While this finding contradicts the study observations by Robinson et al 16 which found depression to be significantly associated with left hemispheric stroke, it coincides with the study findings of Ebrahim et al and House et al17, 4 Recent studies show that psychosocial factors have a greater contribution to the development of post-stroke depression than lesion location. 12, 18, 19
While the literature on post-stroke anxiety remains in the infancy stage, our study could not find any significant association between the prevalence of anxiety and laterality. This finding is in contradiction with that of a study by Astorm etal and Castillo et al 15, 16 which found significant association between anxiety and right hemisphere lesion. There is a scarcity of literature in this area.
Conclusion
The present study attempted to study the psychiatric morbidity of anxiety and depression and socio-demographic variables in patients with stroke. Our study concludes that post-stroke depression and anxiety are mostly seen in the elderly population and males. Majority of cases had left hemisphere involvement. Our study could not establish any association between socioeconomic status, literacy, and the symptomology of the conditions assessed. Our results showed that depression is more among stroke individuals than anxiety. Most of the findings of the current study correlate with earlier studies. Long term studies in a larger population are required to further evaluate post-stroke anxiety in patients and their health-related quality of life.