Introduction
Young stroke is on rise in every part of the world and in significant number of cases, mechanism of stroke remains unknown. So, it is of great importance to address a modifiable risk factor of stroke, to whatever extent possible and at the earliest possible opportunity.
Arterial dissection is a prominent etiology of stroke in young population and increased homocysteine level as a possible precipitating factor is reported in literature.
We will narrate here story of a gentleman who had a bolt from the blue. He had a catastrophic vascular event and increased homocysteine level was the only risk factor detected, probably emphasizing the importance of addressing this vascular risk factor in stroke prevention
Case
A 34-year-old right-handed gentleman, independent at baseline, a pure vegan without any known comorbidities, had a family history of coronary artery disease. He had no addiction and was not on any regular drug. He attended the ER with acute onset vertigo and gait imbalance followed by transient drowsiness which started twenty-four hours before the presentation. There was no history of loss of consciousness, focal weakness or involuntary movement.
There was no systemic complain except vomiting and a holo-cranial dull aching persistent headache since the onset of the symptoms. There was no history of any trauma to head/neck or neck pain. On admission, only bilateral appendicular and axial ataxia were detected with NIHSS of 2.
His MRI brain revealed bilateral acute patchy cerebellar hemispheric infarcts with few focal hits at left posterior parietal lobe.
CT angiography revealed non-opacification of V3 and V4 segments of left vertebral artery without any dissection flap or false lumen. There was no evidence of any other intracranial or extracranial vessel disease either. His biochemical and relevant blood parameters were within normal limits. Patient was managed conservatively with dual antiplatelets and high dose statin therapy considering the large vessel pathology.
He underwent balance and gait training exercises. His tandem walking and appendicular incoordination improved and seven days post admission, he was back to baseline with NIHSS of zero.
His echocardiography was non-contributory, so was the 48hour Holter monitoring. We searched for uncommon causes of stroke and his investigations including vasculitis markers were within normal limit. We also ruled out evidence of deep venous thrombosis in lower limb.
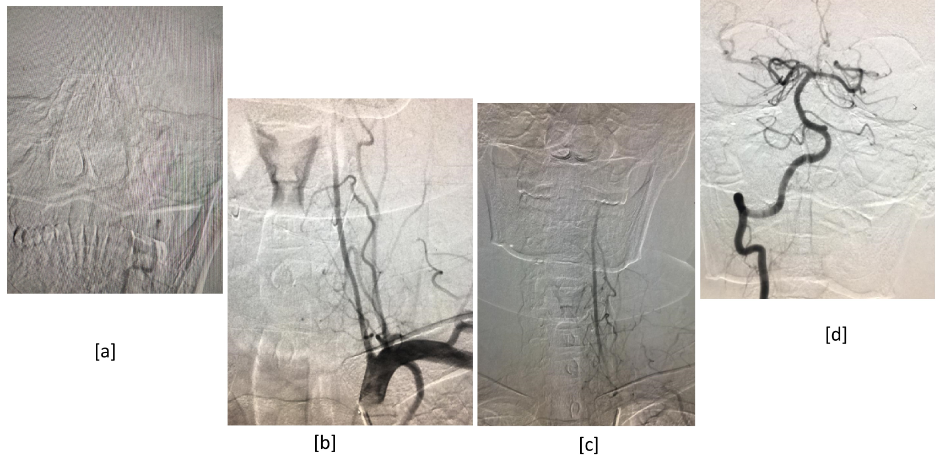
Incidentally we found serum homocysteine level was very high (>50 µmol/L) with low vitamin B12 level. We started vitamin B12, folic acid and pyridoxine supplements for him. He was finally discharged on seventh day with plan for follow up in outdoor. We performed a cerebral DSA on outpatient basis. It revealed progressive smooth tapering of the distal V2 segment of left vertebral artery with evidence of slow flow; there was no visualization of V3 and V4 segment of left vertebral artery suggestive of dissection. Right vertebral artery had normal flow [Figure 1]. So, it was proved that the posterior circulation stroke was attributable to the embolic events from the dissected left vertebral artery.
Discussion
Our young patient had a unique presentation with an isolated spontaneous vertebral artery dissection in association with increased homocysteine level. The points of our discussion should be: whether increased homocysteine level is related to this type vascular event? and secondly, to what extent we need to be concerned if excess amount of this amino acid accumulates inside our body?
In a meta-analysis of 27 trials relating to homocysteine and incidence of vascular events, it was noted that serum homocysteine level above the 90th percentile increases risk for peripheral vascular disease by 6.8 times, venous thrombosis by 2.95, cerebrovascular disease by 2.5 times and coronary artery disease by 1.7 times.1 Approximately, a 5 mmol/L increment in homocysteine is equivalent to 20 mg/dL increment of cholesterol in increasing risk of coronary artery disease 1. Homocysteine probably utilizes its elastolysis activities causing premature breakdown of the arterial elastic fibers. It results into irreversible homocysteine attachment to long-lived proteins especially those with epidermal growth factor - like domains leading to cumulative damage and progressive vascular events.2
Scientists tried finding association between arterial dissection and increased homocysteine level.
In 2002, in an observational study, it was noted that there was a significantly higher level of plasma homocysteine amongst patients with cervical artery dissection. They also noted increased incidence of MTHFR TT genotype amongst patients with coronary artery dissection.3 In a more recent metanalysis it was noted that individuals with the 677TT mutation of MTHFR tend to be associated with increased homocysteine level and cervical artery dissection. Although the mechanism is still unknown, increased homocysteine level probably promotes oxidative stress, vascular smooth muscle cell migration, accumulation of collagen and finally formation of neointima.4 Increased accumulation of this amino acid in-fact acts as a double-edged sword. It is associated with ischemic stroke by inducing atherosclerosis and atherothrombosis on one hand and intracerebral hemorrhage on the other hand by promotion of matrix metalloproteinases-9 (MMP-9) expression, which is responsible for atherosclerotic plaque instability and ruptur.5
Folate, vitamins B12 and B6 deficiency are known to be associated with increased homocysteine level Interestingly, Indians have ten times higher incidence of increased homocysteine level in comparison to global averages.6 In a research conducted at Guwahati, India, it was reported that amongst 110 ischemic stroke patients, increased homocysteine level was detectable as high as 59.1 % of patients.7
There are many vegetarians in India and vegetarian food contains very little vitamin B 12. Milk which is an important part of vegetarian diet contains vitamin B12 but most of it is lost during boiling. Interestingly, Indian vegetarians also have a high incidence of folic acid deficiency. Prolonged cooking is an important reason behind these deficiencies. Studies report that up to one-third of Indians have genetic defect in the enzymes that metabolize homocysteine, especially MTHFR contributing in increased homocysteine level adding another reason for this deficiency.8
No definite guideline exists on optimal approaches to the management of high homocysteine level. Therapy with vitamin B12, folic acid, and vitamin B6 tends to normalize homocysteine by 8 weeks. However, route of administration and the effect on clinical outcome have not been studied in detail. Although, Vitamin Intervention for Stroke Prevention (VISP) trial did not show significant difference in stroke outcome between the groups of vitamin supplementation 9 subgroup analysis showed that patients with high baseline homocysteine who received low-dose vitamins had a higher risk of stroke. Heart Outcomes Prevention Evaluation 2 (HOPE 2) trial showed a less incidence of nonfatal stroke with more than three-year treatment with vitamin supplementation.10
This young gentleman had no known comorbidities except family history of early onset coronary artery disease. We tried to find possible aetiology the of stroke by doing standard investigations and all were found to be non-contributory. Interestingly, homocysteine level amongst his other family members were found to be very high (all of them purely vegetarians). Still, it is difficult to conclude that increased homocysteine level is the reason behind dissection of cranial arteries and may be an incidental finding in our case. This may also be supported by the following evidences:
Patients with increased homocysteine levels have lesions typical of cerebral microangiopathy and usually are associated multiple vessel stenosis and infarctions. Our patient
Brain imaging had no evidence of small vessel involvement, which is commoner association with increased homocysteine level. He presented with spontaneous dissection, a very rare association with this disorder.
Increased homocysteine level with cervical artery dissection has been reported in literature but spontaneous vertebral artery dissection has been very rarely reported in the world literature.
Fortunately, our patient is doing well and had no further attack despite high homocysteine level which is known to be associated with high mortality especially in large vessel disease.
The prevalence of vegetarian diet, genetic predisposition and diet pattern subject Indians to increased chance of increased homocysteine level and may have role in vascular insults. It is a potentially modifiable risk factor for stroke and other vascular events in young population. Although there is still controversy in treating this entity as per western literature, in Indian subcontinent the scenario is different as our foods are not fortified with vitamins like in west. So, we should be cautious about this entity and take necessary steps to screen unaffected family members, detect genetically susceptible persons so that this biochemical abnormality may not have contribution (if any) in future vascular events
.