- Visibility 162 Views
- Downloads 32 Downloads
- Permissions
- DOI 10.18231/j.ijn.2019.019
-
CrossMark

Endoscopic management of third ventricle colloid cysts, analysis of the technical nuances and the neuroendoscopic anatomy: A preliminary experience
Abstract
Introduction: Endoscopic excision of colloid cysts a minimally invasive and highly effective technique in management of third ventricular colloid cyst.
Materials and Methods: Clinical and radiological data of patients undergoing endoscopic colloid cyst excision were retrospectively analyzed in the period July 2017 to August 2018. Operative video were analyzed for the colloid cyst anatomy and the surgical technique used.
Results: Five cases underwent endoscopic surgery during the study period. Three patients had dilated foramen, two patients had retroforaminal type and coapted type of morbid endoscopic anatomy. Gross total excision could be achieved in two patients, two patients had near total excision and one patient had partial excision who had intraventricular bleed which was managed. There was no mortality. All the patients return to their respective jobs postoperatively.
Conclusion: Endoscopic excision is a safe and effective surgical technique for colloid cyst excision. The extent of excision depends on the experience of surgeon and the endoscopic anatomy of the colloid cyst.
Introduction
Third ventricular colloid cyst constitute about 0.5%-1% of all intracranial tumors. There are several therapeutic approach suggested ranging from surgery, shunt, stereotactic aspiration.[1] Due to its location in the roof of third ventricle near the foramen of Monroe, the presentation is usually is biventricular hydrocephalus.[2] The advantage of excellent visualization and minimally invasive corridor through the dilated ventricular system makes endoscopic excision as the preferred treatment of choice in current scenario.[3]
In this paper we present our preliminary experience of five consecutive cases of colloid cysts operated using endoscopic approach.
Materials and Methods
Five cases of colloid cysts were operated in Department of Neurosurgery, J. N. Medical College, Aligarh Muslim University between July 2017 to June 2019. The age of the patient was between 8 years and 60 years.
After taking informed consent all patients underwent endoscopic surgery. We have used Karl Storz lotta hopkins ventriculo scope with wide angled telescope 6 degree, 2.6mm instrument channel and irrigation and suction channel 1.6mm. with high definition camera. Continuous irrigation is done with Ringer’s Lactate .
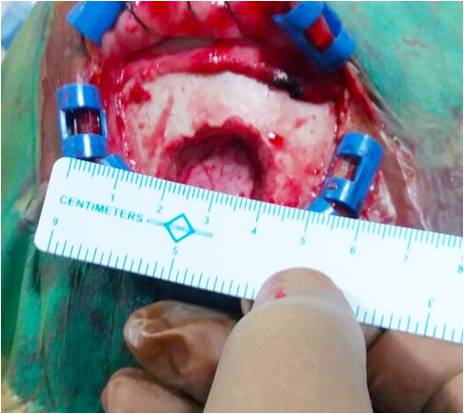
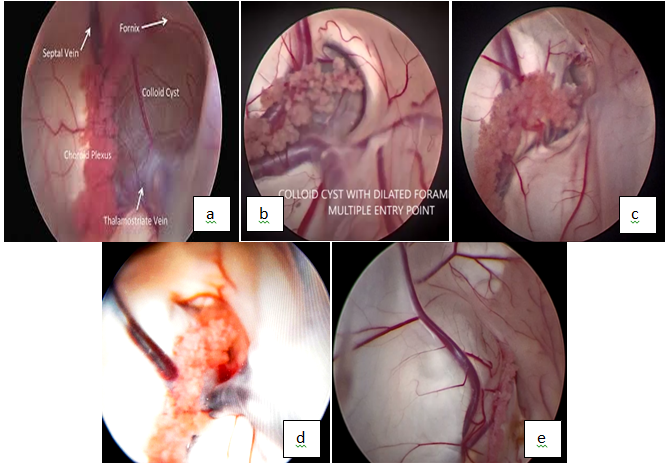
All patient were operated under general anaesthesia. Patients were positioned supine on horse shoe with head end elevated at 30 degrees. Burr hole was made 4cm lateral to midline and 3 cm anterior to the coronal suture [Figure 1]. All patient had moderate to severe hydrocephalus, henceforth free hand technique was used to insert the trocar in all the cases. After checking the ventricular entry zero degree endoscope was inserted and irrigation was started. Anatomy around the foramen of Monroe was carefully defined. Shape of the foramen along with its relationship with Septal and thalamic vein is also defined.[Figure 2]
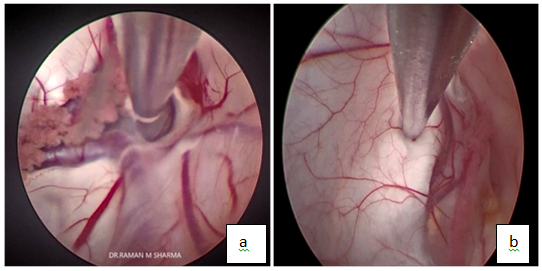
According to the size of the foramen of Monroe and its type two major approach were used (1) Transforaminal Approach (2) Trans- Septal Approach.[Figure 3].
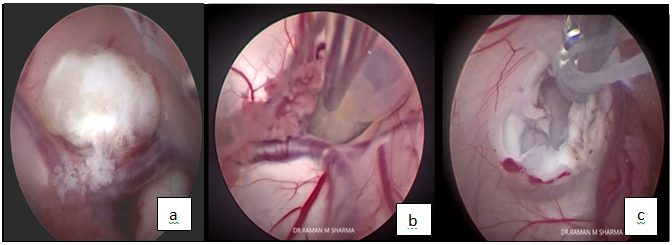
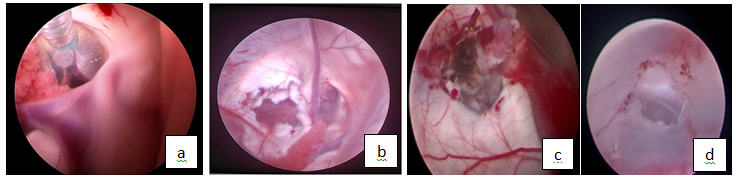
In the transforaminal Approach the foramen is wide and cyst can be seen through the foramen. The cyst wall is coagulated with monopolar along with the feeder arterioles. The cyst wall is cut with a knife and contents are aspirated. Gradual removal of pieces is required with a grasper if the contents are very thick or viscous, in one of the case the content was calcified[2]. Occasionally a fogarthy is inserted and inflated tinside the cavity to widen the opening and press the content out. Once the cyst is decompressed the wall is removed after holding it with biopsy forceps and rotatry movement, piecemeal excision of the cyst wall is preferred. If there is residual cyst wall it is coagulated with bipolar to make it shrink to a very small tissue. Adequate Cerebrospinal fluif (CSF) flow was confirmed at the end of procedure [Figure 5]
In transseptal approach the cyst wall is approached just the anterior or posterior to the septal vein. The same principal of coagulating the cyst wall and aspiration of the cyst content were applied.
Inadverent bleeding was managed with continuous irrigation. If there is bleed from the choroid plexus a tamponade can be applied by 3 French Fogarthy catheter [Figure 5]. Hemostasis is ensured by cauterization of both inner and outer surface of the cyst wall [Figure 5].
At the end of the procedure third ventriculostomy was done in all the case to prevent postoperative blockage of CSF flow by debris and the blood Figure [Figure 5].
Results
Overall five patients of colloid cyst were successfully managed. The youngest patient was 8 year old child and the oldest was 60 years old. Three patients were male two patients were female. Of all five cases three cases presented with intermittent headache associated with blurring of vision and vomiting. One patient had history of drop attacks and headache. One patient has presented with urinary incontinence and walking difficulty. Three patients had colloid cyst measuring more than 2.5cm and two were less than 2.5cm.
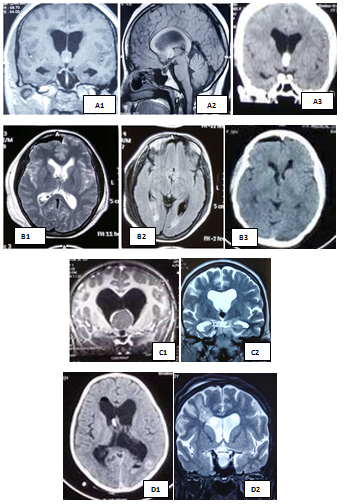
The operative time ranges between 180 minutes to 240 minutes. The type of cyst and the foraminal anatomy defined the approach [Figure 3]. Three patients underwent transseptal or combined approach, two patient underwent transforaminal approach. Gross total excision could be achieved in three patients, two patients had partial excision. Content of the cyst is varied from viscous content, thick and in one of our case the content of collid cyst was calcified [Figure 4].
Two cases had mild to moderate intraventricular hemorrage which required postoperative extraventricular drainage of cerebrospinal fluid (CSF), which was removed within 48-72 hours. One case required postoperative ventriculoperitoneal shunt placement. One patient had transient altered sensorium which improved gradually.
We have a mean followup of 7 months 14 days (range 3mont to 550 days). There was no radiological evidence of recurrence in any of our patient [Figure 6]. All patient return back to their work after an average of 78 days following discharge.
Discussion
The velum interpositum is most likely the site of origin of colloid cyst. They are the slow growing tumors and causes gradual obstruction of the foramen Monroe and hydrocephalus. Because of the enlarged ventricule size and foramen of Monroe these lesion deemed good for neuroendoscopic excision. The cyst either can grow anteriorly which may cause a larger foramen of Monroe and cyst growing in to the lateral ventricle. Such cases are handeled preferably with the direct transforaminal approach.
A cyst growing more posteriorly tends to go medial to the septum pellucidum leading to narrowing of foramen of Monroe. It also leads to widening of interforniceal space and displaces the fornices. Mac Millan described coappted and displayed type of Foramen in such patients. In these cases transforaminal approach is not possible. Aspiration of the cyst content posteriorly and away from the fornices will lead to opening of the foramen of Monroe and subsequent excision of the cyst by transforaminal route. Thus conversion to the microsurgical approach unnecessary. In three of our cases we had to do transseptal approach.[4]
There is a constant debate regarding more incidence of colloid cyst wall residue in endoscopic approach as compared to microsurgical excision. Howsoever there are several studies that suggest that that subtotal resection with cyst coagulation may be sufficient and comparable to microsurgical removal. Hoffman et al in 2017 suggested that residual cyst having high recurrence of 33.3% and the aim of the aim of the surgery to be complete excision.[5] In our series we had two cases in which we could not completely excise the cyst wall. In one of the cases there was torrential bleeding while sepearating the cyst wall from the choroid plexus. We could not excise the colloid cyst wall completely. In this case we have coagulated the wall to shrunk it a small size. Third ventriculostomy and septostomy was done in this patient and extraventricular drain was kept in the postoperative period. Subsequently patient required ventriculoperitoneal shunt for symptomatic hydrocephalus. Both these cases are in followup without any fresh symptoms though the follow up is less than one year. It is to be acknowledge that there is definitive learning curve associated with endoscopic management of intraventricular tumour. It is our initial experience, with the advent of better endoscopic equipment and various endoscopic manoeuvre the excision rates are getting better. We attempt to perform the gross total excision all the case. However we opine that unnecessary traction and manuovere to achieve this goal can lead to uncontrollable bleeding sometime. Good opening of the cyst wall, adequate removal of content and septostomy is recommended in such cases. Biventricular technique has been suggested as a good technique for radical excision.[2]
Source of Funding
None.
Conflict of Interest
None.
References
- Abernathey CD, Davis DH, Kelly PJ. Treatment of colloid cysts of the third ventricle by stereotaxic microsurgical laser craniotomy. J Neurosurg. 1989;70(4):525-529. [Google Scholar]
- Mishra S, Chandra PS, Suri A, Rajender K, Sharma BS, Mahapatra AK. Endoscopic management of third ventricular colloid cysts: eight years' institutional experience and description of a new technique. Neurol India. 2010;58(3):412-417. [Google Scholar]
- Kohama M, Fujimura M, Nagamatsu K, Murakami K, Tominaga T. Neuroendoscopic management of a colloid cyst at the third ventricle using the high-definition flexible neuroendoscopic system: report of two cases. No Shinkei Geka. 2009;37(3):261-267. [Google Scholar]
- A Z, S EK. Endoscopic approach to colloid cysts. Minim Invasive Neurosurg. 2006;49(5):263-268. [Google Scholar]
- Hoffman CE, Savage NJ, Souweidane MM. The significance of cyst remnants after endoscopic colloid cyst resection: a retrospective clinical case series. Neurosurg. 2013;73(2):237-239. [Google Scholar]